



Update: On December 10, 2021, the President signed into law the Protecting Medicare and American Farmers from Sequester Cuts Act. Among its many provisions, the new law delays the effective date for the Radiation Oncology Model to January 1, 2023. You may find our summary of the new law here.
Beginning January 1, 2022, radiotherapy (RT) providers—including physician group practices, hospital outpatient departments, and freestanding radiation therapy centers—in specified zip codes will receive prospective, site-neutral, modality-agnostic, episode-based payments for RT episodes of care for traditional Medicare beneficiaries. On November 2, 2021, the Centers for Medicare & Medicaid Services (CMS) finalized previously proposed modifications to the Radiation Oncology (RO) Model with some minor adjustments in the 2022 Hospital Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) Payment System Final Rule.
The following table summarizes these modifications. As the year winds down, now is the time for affected organizations to execute strategies for success under this mandatory payment model.
| Topic/Category | July 2021 Proposed OPPS/ASC Rule | UPDATED November 2021 Final OPPS/ASC Rule |
| Performance Years (PY) | January 1, 2022 (PY1)–December 31, 2026 (PY5) | Finalized |
| RO Model Exclusion | Participants in the Community Transformation track of the CHART Model or PARHM are excluded[1] | Finalized |
| Low-Volume Opt-Out Criteria | Additionally, a new TIN or CCN is not eligible for opt-out if combined current and legacy entities involved furnished 20 or more RT service episodes across all participating CBSAs in the most recent full year with claims data available prior to the applicable PY[2] | Finalized |
| National Base Rate Calculation Period | 2017-2019 (3 years prior to PY1) | Finalized |
| Case Mix and Historical Experience Adjustment Calculations | CMS will use current and legacy TIN or CCN | Finalized |
| Cancer Type Inclusion | Liver cancer removed, and inclusion criteria adjusted | Finalized |
| Modality Inclusion | Brachytherapy removed from the list of included modalities | Finalized |
| Discount Factor | Professional: 3.5%, Technical: 4.5% | Finalized |
| Payment Amount Subject to Withholds | Quality: 2% of Professional Component (PC)
Incorrect payments: 1% of PC and 1% of Technical Component (TC) Patient Experience: 1% of TC starting PY3 |
Finalized |
| Sequestration Language | 2% deduction for sequestration amended to indicate “sequestration will be applied in accordance with applicable law” | Finalized |
| Qualify as Advanced Alternative Payment Model Under Quality Payment Program | PY1 (2022) | Finalized |
| Alternative Payment Model (APM) or Merit-Based Incentive Payment System (MIPS) Qualifications Updates | Track One: Dual and Professional participants who meet RO Model requirements (including the definition of eligible clinicians and CEHRT[3] use) are eligible for Qualified Participant (QP) determination if they meet the QP threshold; those that do not meet the threshold are eligible for APM scoring in MIPS
Track Two: Dual and Professional participants who fail to meet RO model and monitoring requirements are not eligible for QP determination |
The addition of Track Three: all other participants who would not be an Advanced APM or MIPS APM |
| CEHRT Use Attestation | 30 days prior to PY1 (January 1, 2022) | Finalized |
| Quality Measure Data | No delay; Submit PY1 data in PY2 (March 2023) | Finalized |
| Quality Measure Model Pay for Reporting (PFR) and Pay for Performance (PFP) Periods | Three measures (Pain Plan of Care, Preventive Care and Screening, and Advanced Care Plan) PFP in PYs 1-5;
Treatment Summary Communication measure PFR PYs 1-2 and PFP for PYs 3-5; Patient Experience measures in PY3 |
Finalized |
| CAHPS[4] Cancer Care Survey (For Patient Experience Measures) | Administered PY1 in April 2022 | Finalized |
| Individual Practitioner List (IPL) Review and Certification | Participant must notify CMS of changes to IPL by Quality Payment Program snapshot date (30 days prior to PY) | Finalized |
| Clinical Data Collection Period | Submit PY1 Jan-Jun data in July 2022 | Finalized |
| Incomplete Episodes Payment | For all incomplete episodes where coverage changed during treatment episode, CMS will reimburse with what the fee-for-service rates would have been for those radiation therapy services using no-pay claims | Finalized |
| Reconciliation Payments | Reconciliation calculations and true up payment time periods have not changed; however, quality payments are included in all PYs | Finalized |
| Extreme and Uncontrollable Circumstances Policy | CMS may adjust or waive the performance period, reporting requirements, or pricing methodology, in the event of extreme circumstances | Contingent upon the Secretary’s termination of the Public Health Emergency (PHE) renewal prior to January 1, 2022: 1) collection and submission of quality and clinical measures will be optional in PY1; 2) 2% quality withholding of the professional component will not be applied; 3) requirement to engage with a Patient Safety Organization will be optional; and 4) peer review of treatment plans will be optional |
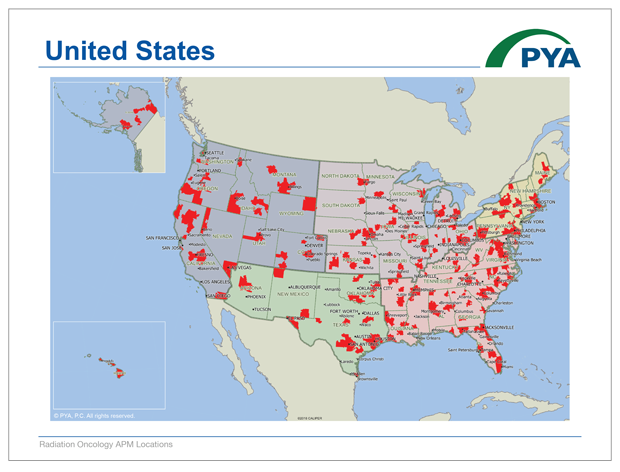
CMS does not propose to change the list of zip codes defining the geographic areas in which the RO Model applies. PYA has converted those zip codes into a map to illustrate the reach of the RO Model.
Click Below to View the PDF Map:
View the Google Map Below (load times vary):
Affected providers should continue planning and implementing strategies for success into the new year:
- Establish a task force of key individuals responsible for staying current on program requirements, managing implementation of any care delivery model changes, collecting and submitting quality measures and clinical data, and addressing the impact on revenue cycle and financial performance.
- Calculate how your current average Medicare reimbursement rate per episode of care compares to RO model rates for the included 15 tumor sites. If your reimbursement is likely to be lower, identify and implement cost-saving measures. For example, consider implementing hypofractionation more consistently for appropriate patients and/or integrating remote patient monitoring to streamline staff utilization.
- Assess your current performance on CMS’ selected quality and reporting metrics, and identify and implement solutions to improve these outcomes.
- Develop and maintain collaborative relationships with providers across the cancer continuum of care by setting common goals and pursuing initiatives to achieve optimum performance under the RO Model.
- Consider pursuing new business models that may better align the hospital and physicians toward common objectives for the RO Model. These may range from integration into a hospital clinically integrated network, medical directorships, or co-management agreements, to professional services agreements or even employment models.
Whether by deploying diversified strategies, differentiating from competitors, or simply improving upon existing strengths, programs will be presented with the opportunity to achieve, and even surpass, their goals. With our deep understanding of the RO Model and wealth of experience helping oncology programs, PYA is here to support your success under this new payment model. For assistance, email one of our executives below, or call (865) 673-0844.
[1] CHART- Community Health Access and Rural Transformation; PARHM- Pennsylvania Rural Health Model
[2] TIN- Tax ID Number; CCN- CMS Certification Number; CBSAs- Core-Based Statistical Areas
[3] CEHRT- Certified Electronic Health Records
[4] CAHPS- Consumer Assessment of Healthcare Providers & Systems


